Brain Reward Circuits, Fibro & Opioids
Treatment & Research News
Brain Reward Circuits, Fibro & Opioids
Home | Treatment & Research News

The potential for reward drives human behavior. Every day you make decisions based on anticipated outcomes, such as more gratification or additional money. No doubt, you also strive for less unpleasantries, especially the alleviation of pain. But in people with fibromyalgia, the brain’s reward and motivation circuits do not work properly. And research involving opioid use provides additional clues about how your brain operates.
“Opioids affect very similar regions in the brain for cognition, attention, pain, mood, and motivation,” says Katherine Martucci, Ph.D., who presented her research to an audience of pain scientists last month.1 Although opioids and chronic pain have been around for a long time, she points out that “we still don’t know much about how opioids interact with chronic pain in the brain.”
Beyond the Status Quo
Almost all brain imaging studies involving chronic pain patients exclude people who are taking opioids, points out Martucci. “Despite this issue, we need to know: How are opioids interacting with chronic pain in the brain?” Without this data, no one knows what long term opioid use does to the brain in chronic pain patients. And if there are any upsides, they need to be explored.
Many of the negative side effects of opioids overlap with the symptoms of fibromyalgia (e.g., fatigue, sleep disruption, brain fog, and constipation). Based on this alone, everyone advises against giving opioids to fibromyalgia patients. “But this is not scientifically based,” says Martucci. “And that’s the main reason why I have focused on opioid use in fibromyalgia.”
But there are obstacles to researching long term use of opioids. “It’s tricky to study,” says Martucci, adding that the potential benefit may be low. “There are risks of addiction and overdose, along with many side effects that could lead to study dropouts. And one could ask: Is it even ethical if you don’t think patients will benefit from opioids?”
Rather than placing fibromyalgia patients on opioids, Martucci is evaluating patients who are already being prescribed these medications. During her speech, she described her brain imaging results for three subject groups. They are (1) fibromyalgia patients who have taken opioids for at least 90 days, (2) patients not taking opioids, and (3) healthy controls.
Opioids Impact Reward Systems
“My lab focuses on brain reward processing because it is altered in chronic pain conditions like fibromyalgia,” says Martucci. “The reward circuity is also involved in the action of opioids, which is why they can be so addictive.”
Martucci’s research tests how her subject’s brains respond to a monetary reward. Participants lay inside an MRI scanner looking up at a screen and holding a clicker in their hand. First, they are presented with a dollar amount they can win. Then they wait in anticipation of a square symbol before they can press the button.
“During the monetary anticipation phase, the healthy controls showed a robust response in their medial prefrontal cortex (MPFC),” says Martucci.2 This corresponded to their anticipation of winning the five dollars. “Whereas the nonopioid patient group showed a deactivation in this region. It’s a blunted response to anticipation of rewards.”
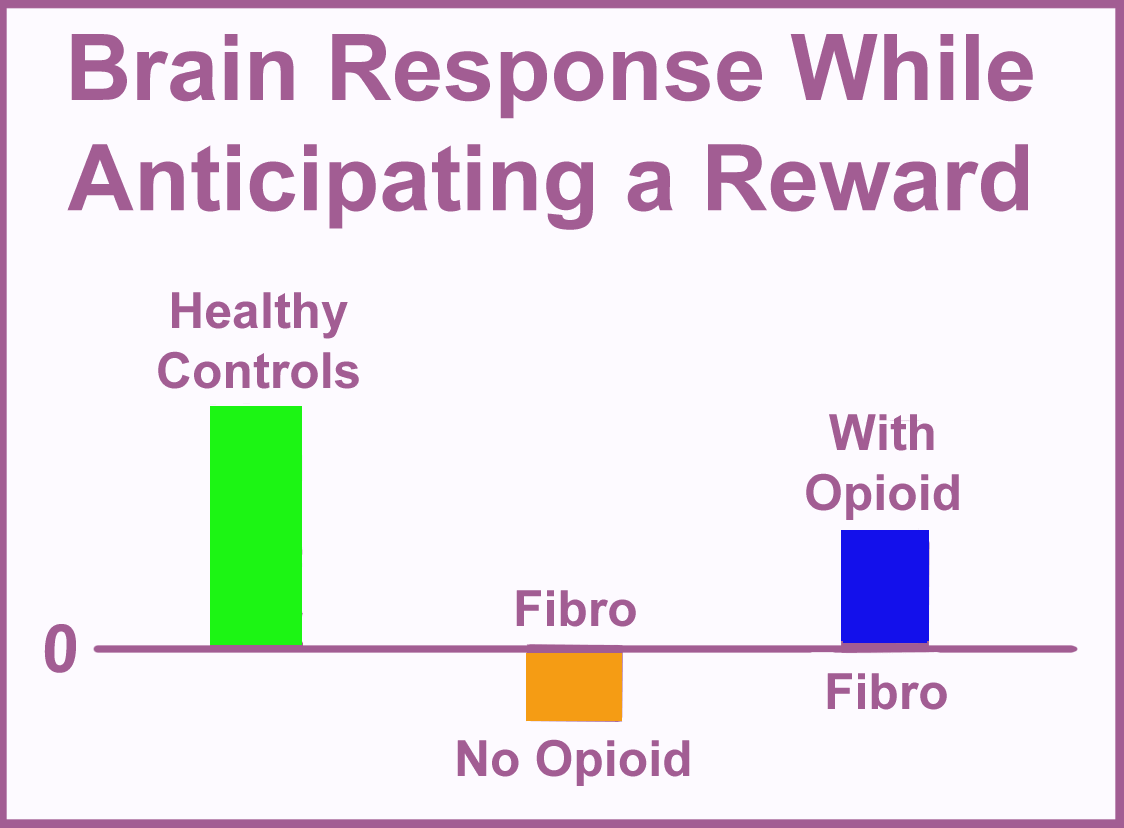
What about the group of fibromyalgia patients taking opioids? Martucci hypothesized that patients on opioids would show an even greater drop in their brains’ MPFC reward response. But to her surprise, she saw the opposite response.
“This indicates that opioids might be helping to somewhat rebalance reward and motivation in fibromyalgia patients who are taking opioids,” says Martucci.
Next, she examined the brain processes involved in reward-related attention.3 After all, your brain must be attuned to a potential reward for it to respond. Martucci looked at two brain centers involved in the attention aspects of reward. These two centers were very actively communicating with one another in the healthy group, but not in the nonopioid patient group.
Looking at the fibromyalgia patients on opioids, the communication between the two attention-related centers was slightly greater (a bit more like the controls). So, it appears opioids might help with the attention aspects of reward processing as well.
Interpreting the Data
Although group differences were detectable, there was a lot of variability between the patients. In addition, many patients had other medical conditions besides fibromyalgia.
“We are crudely comparing events (brain activity in response to rewards) in two patient groups,” cautions Martucci. “We did not compare the same patients under two different conditions (with and without opioids), which is ideal. However, we are answering the question about opioid impacts the best way we can without exposing patients to the risks and side effects of this class of medications.”
The types of opioids, as well as the dose patients were taking, varied significantly. Here is the opioid medication breakdown (number of patients in parentheses):
- Tramadol (5)
- Hydrocodone (7)
- Morphine (1)
- Oxycodone (2)
- Codeine (1)
“In fibromyalgia, the brain reward and attentional deficits may be somewhat reduced by opioids,” concludes Martucci. “But I am certainly not saying, go put your patients on opioids. I think these data show us why some patients do want to stay on opioids because it may be helping to boost their reward system deficits, at least a little bit.”
If you are wondering whether the pain levels, psychological measures or other clinical symptoms were different between the two patient groups, the answer is NO. The opioid effects could only be detected by brain imaging. In other words, the standard tools your prescribing physician relies on to assess the efficacy of opioids will fail to show any benefits.
Hypothetically, if the reward and motivation systems in your brain are less active, it could contribute to other, less tangible symptoms. Reduced ability to act on potential rewards could make it harder for you to feel gratified with your life. Less reward motivation might also compound your fatigue and give others the impression you are depressed.
New Studies Underway
With NIH funding, Martucci is further exploring how opioids impact brain function. Instead of comparing two patient groups (those taking or not taking opioids), she will evaluate brain responses in the same patients at two different time points. First, when the opioid concentration reaches its peak blood level. Next, when the opioid is almost eliminated from the body. This design will provide a more accurate picture of how opioids impact brain function.
“If we can understand how opioids are affecting the brain in fibromyalgia patients, we might be able to identify the mechanisms behind it,” says Martucci. “Then we can target those processes using nonopioid, non-addictive methods to treat the pain and reward systems efficiently.”
Indeed, Martucci is looking to relieve pain and boost the reward system by directly stimulating the MPFC in an AFSA-funded trial. This circumvents any obstacles imposed by opioids and directly targets the defective brain processes in fibromyalgia. For details about Martucci’s transcranial magnetic stimulation (TMS) treatment trial, read more.
Alternatives to Opioids

Opioids are tightly regulated and TMS is in the testing phase, so it is not a treatment option yet. On the other hand, romantic and parental love both activate the brain’s reward centers in healthy subjects. Laughter may also trigger a similar response. Whether these emotions can reduce fibromyalgia pain is unknown but it is worth a try.
Keep photos of loved ones within reach to look at throughout the day. Better yet, put them in a digital picture frame that you keep on your desk at work or wherever you spend most of your time.
Love and affection for pets also stimulates the reward centers. In addition, listening to nostalgic music or songs that you really enjoy might be beneficial as well.
When opioid medications were more commonly prescribed for fibromyalgia, patients often stated: “They take the edge off my pain.” Given the restrictions on opioids today, hopefully some of the above strategies will do the same for you … at least somewhat.
Don’t Miss a Beat on New Treatments & Research: Sign up for a Free Membership today.
Research holds the key to better treatments. AFSA funded six projects in 2024 and 2025; help us fund more in 2026!
Understanding TMS | Medications | Sleep Treatments | Chaos in the Brain
References for Reward Circuits, Fibro & Opioids
- Neuroimaging of Brain Reward Systems: How Opioids Interact with Chronic Pain in Patients with Fibromyalgia by Katherine Martucci, Ph.D., of Duke University, United States Association for the Study of Pain (USASP) meeting March 2026.
- Martucci KT, et al. Sci Rep 9(1):9633, 2019. Free Report
- Park SH, Baker AK, Martucci KT. Sci Rep 25(1):14560, 2025. Free Report