
Pregabalin for Fibromyalgia
Benefits vs. Side Effects
![]()
Pregabalin (Lyrica) was approved by the Food and Drug Administration (FDA) for treating fibromyalgia pain in 2007. Unlike most drugs on the market, large-scale clinical trial data substantiates the use of pregabalin for treating your pain. As a result, there is a 20 percent chance that a physician will hand you a script for this drug.1 But just because a drug is commonly prescribed, it doesn’t mean it’s highly effective or without serious side effects.
If you are handed a prescription for pregabalin, you should know what to expect. First, most physicians will follow the dosing regimen approved by the FDA for this drug, which may not be optimal for you. Second, you need to know if you are experiencing drug side effects or a worsening of your symptoms. But sorting out problems with dosing and the drug’s negative impacts isn’t easy with an unpredictable illness like fibromyalgia. That’s why several physicians provide information about pregabalin and offer tips on reaping the benefits with minimal side effects.
Effectiveness for Fibro
To judge pregabalin’s ability to relieve your pain, you first need to know what constitutes a favorable response. In general, a one-third reduction in symptoms is viewed as providing clinically meaningful relief. It’s also the guideline used by the FDA because patients clearly notice this degree of pain relief.
The data from the FDA trials using pregabalin to treat fibromyalgia is deceptively impressive. Roughly 42 percent of the patients reported a one-third reduction in pain on the drug. However, 33 percent of the patients taking the placebo (sugar pill) also reported this same degree of benefit.2 This information is based on patients taking the drug at 300 mg/day. For patients at the higher dose of 450 mg/day, the degree of pain reduction improves by 5 percent. However, the side effects also increase.
What are the odds that pregabalin will effectively treat your fibromyalgia pain? There is a 1 in 11 chance that you experience a substantial symptom benefit from the drug.3 But that’s not all. The authors of this summary report offer an important perspective on pregabalin. “Patients should be made aware that they are equally as likely to experience intolerable adverse effects from the drug as they are to experience substantial benefit.”
Given the low odds that pregabalin will effectively treat your fibromyalgia, why bother with it? There is a substantial amount of data on this medication from over 2,000 patients and the response varies tremendously. Some fibromyalgia patients claim, “I got my life back.” Others state, “Pregabalin did nothing for me but produce intolerable side effects.” The only way to know if you fall into the “responder” group is to give the drug a try.
FDA Guidelines
The recommended dosing of pregabalin for fibromyalgia patients goes as follows:
- Start at 75 mg twice a day for the first week (150 mg/day total)
- Increase to 150 mg twice a day for the second week (300 mg/day total)
- If the drug is tolerated and the patient does not notice a 30 percent reduction in pain, increase the dose to 225 mg twice a day (450 mg/day total)
Most patients find this standard dosing regimen too aggressive and cannot tolerate the 450 mg/day dose. However, you can modify the way you take pregabalin to circumvent some of the side effects. In addition, settling on a lower dose can still offer pain relief and improve your sleep. This is why four physicians experienced with prescribing pregabalin for their fibromyalgia patients offer the advice in the sections below.
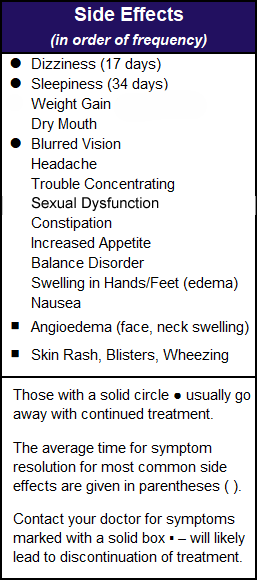
Common Side Effects
Most of pregabalin’s side effects are dose dependent. In other words, the more you take the greater your chances of getting a particular side effect.4
“The most common reasons for discontinuing pregabalin are sleepiness and weight gain,” says Kenneth Miller, M.D., of Danbury, CT. “Blurred vision occurs in less than 10 percent of patients and usually resolves with continued use of pregabalin.” If you encounter this side effect, notify your doctor. You need to have routine eye exams as a precautionary measure. “Dry mouth and constipation occur more often at the higher doses,” adds Miller. The cause of these two side effects is unknown.
Weight gain can plateau after four months or it can take two months for this side effect to occur.5 The average weight gain per month for patients at the 300 mg/day dose could be as high as 4.5 percent of a person’s body weight. “I have seen patients gain 10-15 pounds during the first 3-4 months,” says Miller. “If a patient gains more than this, I advise discontinuing the drug. Pregabalin increases appetite, so patients must monitor their calories and increase physical activity.”
“Patients who get edema (fluid retention) can try taking a mild diuretic,” says Miller. In fact, Lesley Arnold, M.D., of Cincinnati, OH, says she starts patients with an over-the-counter diuretic, such as pamabrom, but she has had mixed results. “It’s the active ingredient in the PMS drugs and you can find it sold separately in the diet section of the drugstore,” says Arnold. “If a patient has a good response to pregabalin but the fluid retention is uncomfortable, diuretics are worth a try.”
Sexual dysfunction occurs within weeks of using pregabalin.6 Neither erectile dysfunction nor loss of libido is dose related. These side effects resolve with discontinuation.
Nighttime Dosing
 I. Jon Russell, M.D., Ph.D., of San Antonio, TX, suggests that patients take pregabalin at bedtime to minimize dizziness. In addition, he uses the sedating side effect to help with sleep. This strategy makes sense given that studies show pregabalin improves the quality of sleep in fibromyalgia patients.7 In fact, it boosts the sedating brain chemical, GABA, while it reduces sleep-disrupting glutamate.8 However, if you only take pregabalin at night, will you get enough pain relief during the day? Also, can this approach minimize any of the other common daytime side effects?
I. Jon Russell, M.D., Ph.D., of San Antonio, TX, suggests that patients take pregabalin at bedtime to minimize dizziness. In addition, he uses the sedating side effect to help with sleep. This strategy makes sense given that studies show pregabalin improves the quality of sleep in fibromyalgia patients.7 In fact, it boosts the sedating brain chemical, GABA, while it reduces sleep-disrupting glutamate.8 However, if you only take pregabalin at night, will you get enough pain relief during the day? Also, can this approach minimize any of the other common daytime side effects?
“I have many patients that get an entire day of symptom relief when they just take pregabalin at bedtime,” says Kevin Hackshaw, M.D., now at the University of Texas in Austin. “I would say there is a 50 percent chance that this strategy will be effective.” He adds that predominant nighttime dosing leads to less daytime side effects for the other problems listed in the table.
Using this strategy, blurry vision and dry mouth shouldn’t bother you during sleep. Also, edema (especially swelling in the legs) ought to be lessened because you are not on your feet when the higher dose of pregabalin is in your system. Taking the brunt of pregabalin at night gives your GI system a break from the drug during the daytime. This makes constipation problems less likely.
Even if you find nightly dosing of pregabalin helpful, Hackshaw says, “It is more often effective for fibromyalgia as an all-day medication.” But how do you get around the daytime side effects? In the next section, Hackshaw provides a dosing strategy that is geared to minimize side effects.
Tailored Approach
How can you achieve daytime pain relief without getting knocked out by the daytime side effects? Hackshaw places his patients on 25 mg in the morning, 25 mg in the late afternoon, and then anywhere from 100 to 150 mg at bedtime. “You don’t have to take the 150 mg dosage two times a day to get relief from pregabalin.”
Sometimes Hackshaw writes two prescriptions, one for 25 mg capsules of pregabalin to be taken twice daily, and a separate script for 150 mg capsules to be taken at bedtime. This method may be the most convenient for patients and is usually covered by insurance companies, but it requires patients to pay for two copays. This approach is more costly, but now that pregabalin is available as a generic, it may be doable.
“A way to get around the issue of two copays is to write just one prescription for 25 mg caps,” says Hackshaw. “For example, I write the script for one 25 mg cap in the morning, one 25 mg cap in the afternoon, and six 25 mg caps at bedtime. Insurance companies usually approve prescriptions written in this manner. The advantage of this prescription is that you only pay one copay because the copay is dependent on the different dosages of pregabalin and independent of the number of capsules being dispensed.”
Certainly, the above dosing strategy in which the brunt of pregabalin is taken at bedtime with small booster doses during the day, is bound to minimize side effects. It also makes plenty of sense to increase nighttime dosing to improve sleep. So, why is this dosing method of using pregabalin for fibromyalgia not publicized? Drug manufacturers are required to adhere to the FDA-approved dosing schedules (e.g., 150 to 225 mg twice daily).
Real World Dosing
If you tried pregabalin but the side effects prevented you from reaching the recommended daily dose of 300 to 450 mg, you may be a typical fibromyalgia patient.
Daniel Arkfeld, M.D., and his team at the University of Southern California, evaluated a series of 126 fibromyalgia patients who were treated with pregabalin in clinical practice.9 He wanted to determine how many tolerated the recommended dose of 300 to 450 mg pregabalin per day.
Unlike the fibromyalgia patients in the treatment trials for pregabalin, these patients were likely taking several other medications. Many also had other medical conditions, so they represented the typical patient.
Out of the 126 patients, 113 were able to tolerate pregabalin. However, the average dose achieved with continued therapy was only 150 mg/day, and this was also the most frequently used dose. Only seven patients were able to tolerate the FDA approved dose of 300 mg/day and one patient was able to handle the higher recommended dose of 450 mg per day.
In a larger study involving 915 patients, the average pregabalin dose was 160 mg/day. The point is, if you find pregabalin beneficial at a lower dose, your response to this drug is quite normal. As with many medications prescribed for fibromyalgia, higher doses generally don’t offer more benefits; just more side effects.
- To learn about other medication options, see Medications.
- If you are curious about nondrug approaches, see Alternative Therapies.
Symptoms | What Is Fibro | Finding Doctor | Muscle Pain Relief | Fibro Friendly Exercises
Stay Current on Treatments & Research News: Sign up for a Free Membership today!
References for Fibromyalgia Pregabalin
- Rico-Villademoros F, et al. Clin Exp Rheum 38(Suppl 123):S72-S78, 2020. Free Report
- Silber AC, et al. J Pain 12(4):407-15, 2011. Free Report
- Donnelly L, et al. Am Fam Physician 97(9):online, 2018. Free Report
- Mease PJ, et al. J Rheumatol, 35(3):502-14, 2008. Abstract
- Arnold LM, et al. Postgrad Med 129(8):921-933, 2017. Abstract.
- Hamed SA. Clin Neuropharmacol 41(4):116-122, 2018. Abstract
- Roth T, et al. Clin J Pain 32(4):308-12, 2016. Abstract
- Harris RE, et al. Anesthesiology 119(6):1453-64, 2013. Free Report
- Arkfeld DG, et al. American College of Rheumatology Meeting San Francisco, 2008.